
Surgical Management of Traumatic Facial Paralysis
Introduction
Facial paralysis has immense psychological impact on patients due to cosmetic deformity. It also has physical morbidities like inadequate eye closure, exposure keratitis. Common causes of facial palsy are bell’s palsy, traumatic facial palsy and tumor. Most common causes of traumatic facial palsy are temporal bone fracture (Road traffic accident), penetrating injuries (Gunshot) and iatrogenic injuries (ear surgery). Injury of facial nerve in temporal bone fracture can result from compression from bony fragments, intraneural hematoma and edema of facial nerve. HRCT of temporal bone is the gold standard investigation to identify potential sites of injury to the facial nerve. Surgery (facial nerve decompression) is the mainstay of treatment of unresolved facial nerve palsy.
A Case Report
A 40 year old male presented with facial asymmetry following a road traffic accident one month back.
Treatment History:-
The facial paralysis did not subside even after one month of conservative management.
On examination:- There was facial disfiguring, incomplete eye closure (Right side), loss of forehead wrinkles. The patient had grade IV facial palsy right side based on House-Brackmann grading.
Investigations:-
Pure tone audiometry :-Mild conductive hearing loss
Schirmer Test (Topodiagnostic test) was done which was positive in the right eye.
HRCT temporal bone:-Fracture in Vertical and Tympanic segment of facial nerve (Fig. 1).
MRI:-No facial nerve transection, Facial nerve oedema.
Surgical management:-
Various approaches can be used for facial nerve decompression including middle cranial fossa approach, trans-mastoid approach, transcanal approach depending on the site of injury. We operated this patient through a trans-mastoid approach using both microscope and endoscope.
STEPS:-
1. Patient was operated under G.A. a 3mm 0 degree Hopkins Rod Endoscope was used using Karl Stortz HD monitor.
2. Right post aural incision was given.
3. Canal wall up mastoidectomy with extended facial recess was performed.
4. Bony fragments impinging on the facial nerve (vertical part) was removed.
5. Vertical part, second genu and horizontal part of facial nerve was exposed completely keeping the ossicular chain intact.
6. The exposed facial nerve was covered with temporalis fascia graft.
Post operative management:-
Injection, Dexamethasone was given for 5 days.
Physiotherapy was done for 3 weeks.
After 3 weeks facial paralysis was improved from grade IV to grade II.

Assistant Professor, Department of ENT, KIMS, Bhubaneswar

Conclusion:-
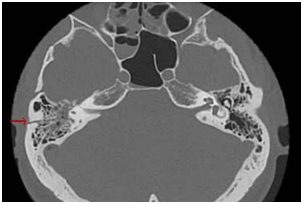
fracture line in right side
Patients with facial palsy due to road traffic accidents usually have late presentation to the ENT surgeon. To get the best results, a patient should be operated upon within 3 weeks of trauma. Use of endoscope in this surgery has added advantage of clear visualization, preservation of hearing and assessment of surgical sites. Post operative physiotherapy has an important role in getting good results.