
Surgical Management of Glomus Jugulare Tumor: An Infratemporal Fossa Approach
Introduction
Paragangliomas (commonly referred to as glomus tumors) are tumors of the paraganglionic tissue. They are slow growing, usually benign and highly vascular tumors. Within the head and neck, these cell rests are predominantly distributed throughout the middle ear in close association with Jacobson’s nerve [branch of cranial nerve (CN) IX], Arnold’s nerve (branch of CN X), the jugular foramen, vagus nerve and carotid body.
Within the temporal bone two types of paragangliomas exist: glomus tympanicum and glomus jugulare. Glomus tympanicum arises from rests of paraganglionic tissue associated with Jacobson’s and Arnold’s nerves. Glomus jugulare is believed to arise from similar paraganglionic rests within the adventitia of the jugular bulb, intimately associated with CN IX, X and XI.
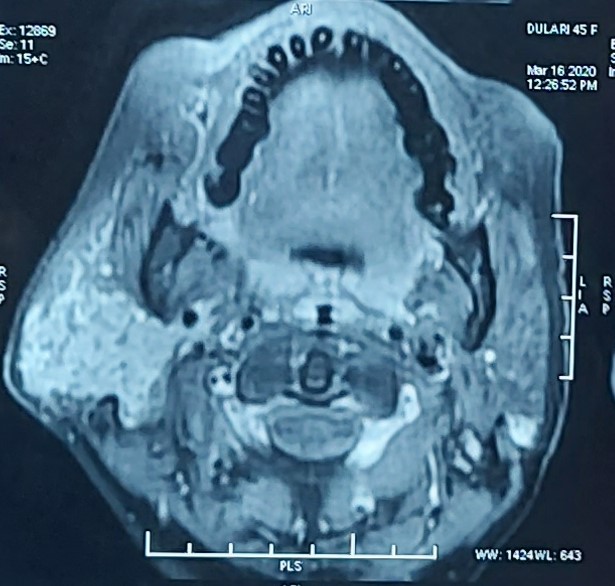
Glomus jugulare tumors are associated with an irregular erosive enlargement of the jugular plate (floor of the hypotympanum) and the jugulo-carotid spine, resulting in a pattern described as “moth-eaten”. In Magnetic resonance (MR) weighted images on T1 weighted images (T1WI), paragangliomas appear hypo intense with a speckled appearance. On gadolinium enhanced T1 images, they demonstrate early and pronounced enhancement. On T2WI, paragangliomas are hyper intense and when larger than 2 cm, they demonstrate a serpentine flow void pattern described as “salt and pepper” appearance. In angiography, paragangliomas exhibit an intense blush or a “bag of worms” appearance.
Case Illustration
A 52-year-old woman attended the otorhinolaryngology (ENT) outpatient department of Kalinga Institute of Medical Sciences (KIMS) with a history of right-sided severe tinnitus, hearing loss and otalgia. No acute distress, speech was normal to conversation. Gait and balance testing revealed a normal tandem walk and negative Romberg sign. There were no motor, sensory, or reflex deficits. Upper cranial nerve examination was unremarkable, the face was symmetrical at rest. Swallowing was grossly normal. There was no tongue atrophy. The palate and the uvula were in the midline, and the sternocleidomastoids had normal tone and function. There was no evidence for Horner’s syndrome.
Otoscopic examination revealed a red mass projecting from the external auditory canal from right side, a normal left ear, and no cranial nerve deficit. There were no other neurological or otological findings. Blood pressure was 130/80, pulse was 86 beats per minute, and there were no symptoms or signs of catecholamine excess. Initial investigation consisted of pure tone audiometry, which showed a right-sided conductive hearing loss with a mean bone conduction threshold of 50 dB and a mean air conduction threshold of 27 dB. Imaging investigations included computed tomography (CT) and gadolinium-enhanced magnetic resonance imaging (MRI), which revealed a 82 mm enhancing mass which was vascular present at the right jugular foramen, middle ear extension, mastoid and sigmoid sinus and internal jugular vein extension with salt and pepper appearance. Urinary noradrenaline excretion was 580 nmol in 24 hours (normal range < 601) and plasma normetanephrine was 985 pmol/L (normal range < 1,180), but other urinary and plasma catecholamines were within normal limits.
Successful resection of glomus jugulare tumors requires an extensive battery of preoperative testing because of the abundant vascularity, deep location, complicated anatomy of the skull base and difficult surgical approach and hence examination was done in detail by Professor Dr. Khageswar Rout and patient was taken up for surgery.
Management
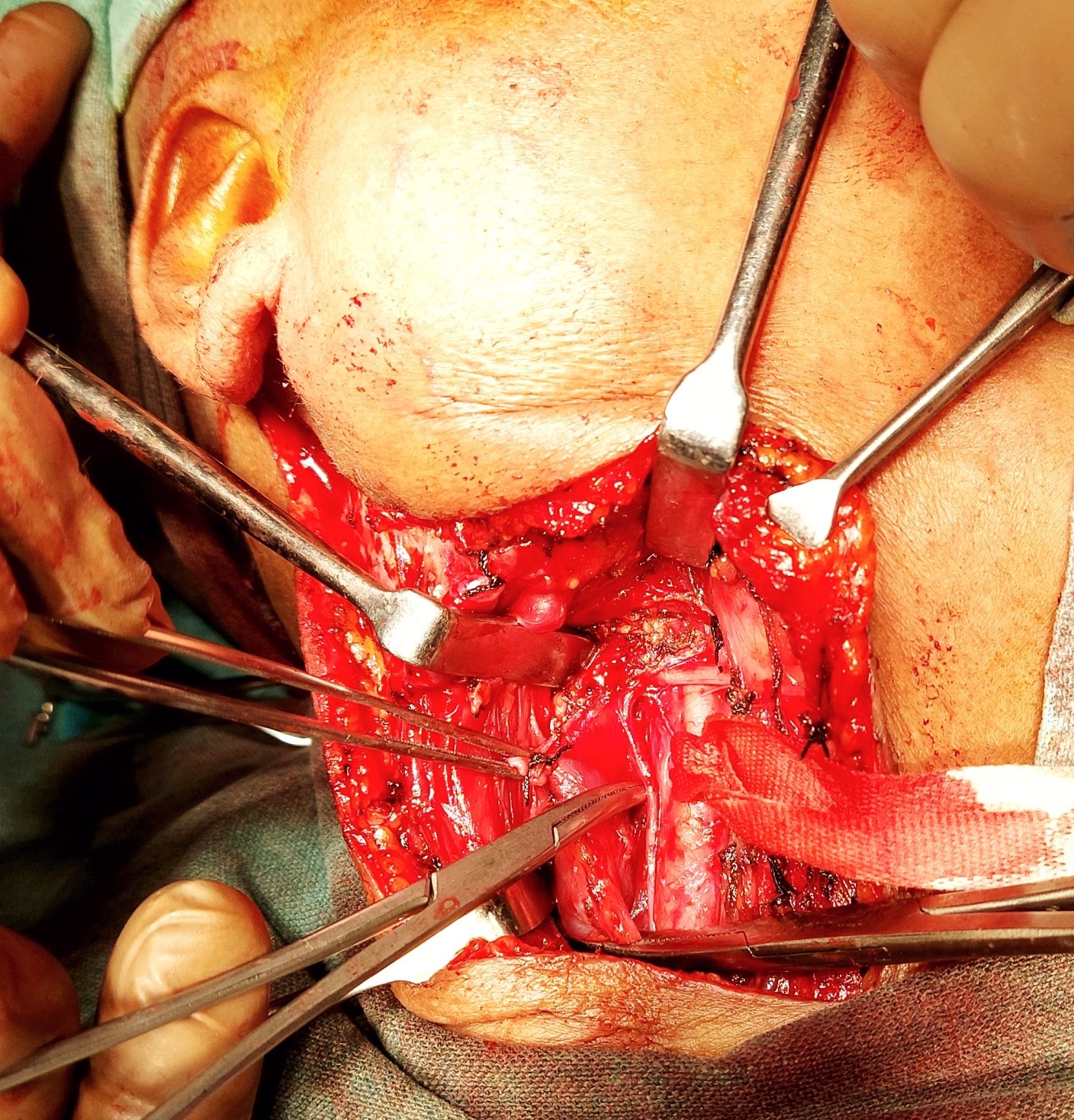
Following routine preparation, positioning, and registration, an incision was made over the right infra-temporal, post aural extending up to the right supraclavicular region medial to sternocleidomastoid muscle. Following meticulous neck dissection, internal jugular vein was ligated, radical mastoidectomy was performed with amputation of the mastoid tip. Following satisfactory exposure and with control of bleeding, the tumor was approached from inside the Jugular foramen and a highly vascular bulky tumor was found in mastoid antrum, middle ear eroding the sigmoid sinus plate was cauterized and removed. Occlusion of sigmoid sinus done with bone wax. Facial nerve transposition done. Ossicles were removed. Total debulking of tumor done.
The most common complication following surgery involves worsening of lower cranial nerve function. Large tumors have an increased risk of brain stem involvement causing vocal cord paralysis. Hence tracheotomy was done to prevent aspiration.
Due to the extensive surgical time (greater than 8 hours), blood loss, and edema, the patient was kept sedated and intubated overnight with hourly neurological vital signs monitoring and continuous arterial blood pressure monitoring. Following extubation, she was alert and moving all extremities.
She had mild ataxia, increased hearing loss on the right, mildly worsened dysphagia, and a partial facial palsy. Dexamethasone, was started intraoperatively, and was maintained for a week and then gradually tapered. Rehabilitation included speech/ swallowing therapy, gait training, plus treatment directed towards maximizing facial nerve recovery including massage, and facial exercises. By the first office visit 4 weeks after surgery, the patient demonstrated improvement of the facial palsy, had returned to near preoperative level of dysphagia, and had minimal ataxia. Continued gradual lessening of all deficits is expected. The MRI will be repeated annually for the next few years.



This challenging and life saving procedure was made possible by the best efforts of Doctors of KIMS from the Department of ENT during the Covid-19 pandemic. The leading surgeon was Dr. Khageswar Rout assisted by Dr. Pradipt Ranjan Sahoo, Dr. Himanshu Mishra, Dr. V. Rachit , Dr. Shubham Agrawal.