
Foreign Body Glottis: A Rare Case in Challenging Times
By Dr. Saswati Das, Asst. Prof.; Dr. Ayesha Pattanaik, Senior Resident; Dr. K. Ranjitha, PG III; Dr. Shambhavi Tiwary, PG II, Dept. of Anaesthesiology, KIMS
Introduction
Foreign body aspiration with asphyxiation is one of the leading causes of accidental deaths among children below four years. Laryngeal foreign bodies are rare (2-5%) in the pediatric age group in comparison to bronchial foreign bodies. Narrow laryngeal air column in children causes hindrance to intubation and ventilation, moreover laryngeal oedema develops quickly by the trauma and the tissue reaction caused by foreign body. Complication rates for bronchoscopy and the laryngotracheal foreign body itself increase with the duration of the foreign body in situ. Because the passage of an endotracheal tube is not possible, the airway is never secure. Therefore, there is the constant danger of complete airway obstruction during manipulation of the foreign body. The nature of the fb to the age of the child in this COVID pandemic made it an interesting case for discussion.
Case Report
A 13-month-old male child presented to the emergency department of our hospital at 12.30 am with complaints of sudden onset of cough followed by noisy breathing after alleged history of unknown foreign body ingestion with shortness of breath. The child tested negative to Rapid antigen testing and therefore shifted to the isolation unit of PICU for further management. On examination the child was irritable and crying. There was tachypnoea with inspiratory stridor and chest retractions. His SpO2 on room air was 78% but progressively increased to 100% with Oxygen @10L/min with facemask. On auscultation breath sounds were audible on both sides. Systemic examination did not reveal much except for tachycardia (HR = 160bpm). A chest X-ray PA and lateral view was done showing a radio-opaque foreign body at the larynx. An emergency bronchoscopy and foreign body removal under general anaesthesia was planned after ENT consultation.
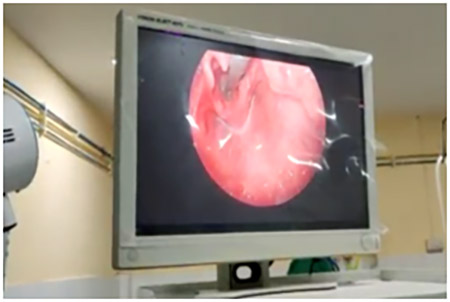




As the RT-PCR reports were pending, we decided to conduct the procedure in the OT of the isolation unit. Though we had a lot of experience in fb removal, the challenges of performing them wearing the PPE could not be undermined. The child was nebulised with adrenaline in the pre-operative area before shifting him to the OT. Inj.Hydrocortisone 25mg and Inj.Dexamethasone 2mg were given i.v. All routine monitoring (electrocardiogram, pulse oximeter, noninvasive blood pressure) were attached. The child was placed in a supine position with an extended neck by placing a shoulder roll. We decided to proceed with inhalational induction using Sevoflurane with 100% Oxygen. All the preparations were made to carry out emergency tracheostomy or cricothyrotomy, if necessary. Despite our best efforts, the ventilation was not adequate though the SpO2 never fell below 98%. Though the risk of contamination by droplets is higher in spontaneously breathing patients, we avoided using a muscle relaxant for the fear of losing the airway. Also bag and mask ventilation would further dislodge the fb. Once the child was adequately anaesthetised rigid bronchoscope was introduced under direct laryngoscopy. We noticed a green colored fb (rusted metal chip) at the glottis which explains the inadequate ventilation despite our best efforts.
We attempted holding the foreign body using curved artery forceps but while retrieving it, the foreign body broke into two parts and the other part slipped into the nasopharynx. We immediately intubated the patient with an uncuffed 3.0mm ET tube. Anaesthesia was maintained on Sevoflurane with 100% 02 and Inj.Atracurium 5mg. The foreign body from the nasopharynx was then easily retrieved using the bronchoscope.
The vitals were maintained throughout the procedure but we planned to shift the patient to PICU for elective ventilation fearing glottic edema. The patient recovered well and was extubated in the evening.
The removal of a laryngeal foreign body under general anaesthesia is a difficult and hazardous task more so while wearing PPE. A good teamwork between the otolaryngologist and anaesthetist to maintain the airway at all times is very essential. We were able to do such challenging procedures under the tutelage of our HOD Brig. Prof. Dr. G. C. Satpathy. We would also like to congratulate Dr. Khageswar Rout, Dr. Ayan Maity and Dr. Ananya Patra from the department of ENT for meticulous retrieval of the fb and amazing teamwork.