
Challenging Cases in Urology A Rare Large Adrenal Myelolipoma Managed Laparoscopically in KIMS
“The skills of a surgeon are tested by challenging cases”- We acknowledge that all patients are important and present with certain challenges regarding diagnosis and management but some cases are more complex, hence need experience and expertise for their management. The Department of Urology, KIMS presents a series of papers describing such challenging cases treated at the Department.

By Dr. Sumanta Kumar Mishra, Assistant Professor, Department of Urology, KIMS
Introduction
Adrenal myelolipomas (AMLs) are rare, benign neoplasms of the adrenal gland with varied clinical presentations. AML was first described in 1866 by Arnold but myeloid component was described in 1905 by Gierke[1]. The incidence was rising in the last two decades due to increased use of imaging modalities like ultrasound and CT scan for varied reasons. AMLs are most commonly seen in fifth and seventh decades of life and are equally prevalent in both sexes. They are generally non secreting tumors and diagnosed by radiological imaging like CT scan and MRI. Small AMLs were detected as adrenal incidentaloma but large ones like “Giant AMLs” which is defined as tumors larger than 10 cm, usually presents with features of pressure effect on surrounding structures and occasionally as acute abdomen due to spontaneous rupture. In asymptomatic small tumors, conservative management is sufficient but surgical intervention is needed for large, symptomatic tumors or when associated with secreting components. Minimally invasive surgery is increasingly used for small AMLs but is challenging in cases of giant AMLs. The rarity of these tumors precludes any case-controlled or randomized study into their management. The available literature is limited to case reports and short series from referral centers. We are presenting such a case of giant AML managed by laparoscopic adrenalectomy in our institute.

Case Report
A 49-year old lady was presented to the Urology Clinic in KIMS with dull aching left flank pain and dyspepsia for the last 3 months. She was diabetic for 2 years on oral hypoglycemic and hypertensive for the last 5 years on medications. She had LSCS 16 years back and attained menopause 2 years back. She doesn’t have palpitation, headache, dizziness, pedal edema or any recent weight loss or weight gain.
Physical examination: She had central obesity with BMI of 37. On examination, her systemic blood pressure was 160/90 mm of Hg, pulse 80/min and no abdominal mass palpable.
Evaluation: Her ultrasound abdomen showed a well-defined brightly echogenic lesion measuring 82x92x117mm seen in the left adrenal region. Her blood investigations including serum electrolytes were normal. Contrast enhanced CT scan with adrenal protocol showed Large retroperitoneal mixed density lesion of size 9.8x 7.3x 9.5 cm noted in the anatomical side of the left adrenal gland displacing left kidney downwards (Fig 1,2). Lesion contains gross fat density area with some soft tissue density area suggestive of adrenal myelolipoma. Right adrenal was normal. Her endocrine evaluation was done to rule out secreting tumours including pheochromocytoma. All hormonal evaluation including 24 hours urinary metanephrines and normetanephrines, serum cortisol, DHEAs, serum aldosterone and renin levels were within normal limits.
Treatment: Based on radiological features and hormonal evaluation she was diagnosed with left adrenal myelolipoma. After proper counseling the patient about the treatment plan laparoscopic left adrenalectomy was planned.
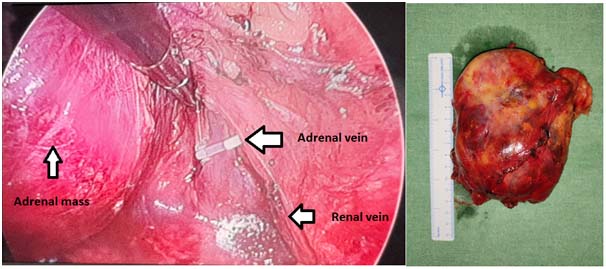
Procedure: Standard three ports were placed by Hasson’s technique in right lateral decubitus position and adrenal approached by transperitoneal route. Key steps of surgery were identifying and controlling the adrenal vein while safeguarding the renal hilar vessels along with spleen and pancreatic tail (Fig 3,4). The adrenal mass of 11 x 9 x 9 cm was excised and retrieved by a pfannenstiel incision. The patient was discharged on 3rd postoperative day.
Pathology Report: Adrenal mass of 15 x 2.5 x 5 cm with normal adrenal tissue of 2.5 x 2 x 1.5 cm on one side. Sections showed sheets of adipose tissue and hematopoietic elements showing trilineage haematopoiesis suggesting adrenal myelolipoma.
Discussion: Adrenal myelolipomas are rare and mostly detected as adrenal incidentaloma (AI). They are second most common findings in AIs next only to adrenal adenoma. Giant adrenal myelolipomas are rarer and about 51 cases reported in literature[2]. AMLs of size less than 4 cm were kept on follow up while larger tumours need surgical excision[3]. Laparoscopic adrenalectomy is more commonly done in expert centers and about 21 cases of giant AML being operated laparoscopically being reported[4]. Our patient had such a giant AML and presented with features of pressure effect due to mass. Her hypertensive status and central obesity warranted for hormonal evaluation which were normal and helping confirming diagnosis. Although this is a benign lesion, surgery is needed in large symptomatic cases and suspicion of malignancy. AMLs doesn’t recur after surgical excision with recurrence free survival rate up to 12 years being reported [5].
Conclusion: Management of AIs is evolving. Metabolic work-up should not be avoided on the basis of CT/MRI findings of AML. Increasing experience in laparoscopy has made minimally invasive surgery acceptable for giant AMLs. However, more research and evidence are needed before this procedure can be recommended for giant AMLs.
References:
1. Plaut A. Myelolipoma in the adrenal cortex; myeloadipose structures. Am J Pathol1958;34:487-515
2. Song JH, Chaudhry FS, Mayo-Smith WW. The Incidental Adrenal Mass on CT: Prevalence of Adrenal Disease in 1,049 Consecutive Adrenal Masses in Patients with No Known Malignancy. AJR Am J Roentgenol2008;190:1163-8.
3. Zeiger MA, Thompson GB, Duh QV, Hamrahian AH, Angelos P, Elaraj D, Fishman E, Kharlip J; American Association of Clinical Endocrinologists; American Association of Endocrine Surgeons.The American Association of Clinical Endocrinologists and American Association of endocrine Surgeons medical guidelines for the management of adrenal incidentalomasEndocrPract. 2009 Jul-Aug; 15 Suppl 1:1-20.
4. Shenoy G. et al, Adrenal myelolipoma: Controversies in its management.Indian Journal of Urology, Apr-Jun 2015, Vol 31, Issue 2
5. Ionnidis O, Pappaemmanoilu s, Chatzopoulos s, et al; Giant bilateral adrenal myelolipomas associated with congenital adrenal hyperplasia; Patholoncol Res 2011