
Endoscopic Ultrasound Guided Cysto- Gastrostomy in Disconnected Pancreatic Duct
By Dr. Venkata Jayadeep Devisetty, Senior Resident (DM), Department of Gastroenterology & Hepatology, KIMS
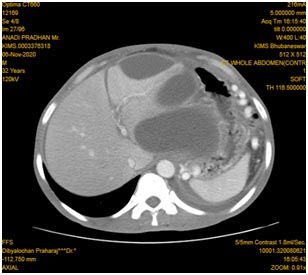
A 32-year old male patient was presented with pain in his abdomen for three years. The pain was intermittent, localized in the epigastric region, moderate to severe in intensity and radiating to back. He had significant loss of appetite and loss of weight. He had a history of ethanol use disorder for the last eight years. Contrast enhanced CT of the abdomen showed features of chronic calcific pancreatitis with multiple large stones in parenchyma and main pancreatic duct (MPD) in the head region with upstream dilatation of MPD and disruption of MPD in distal body region (fig 1).


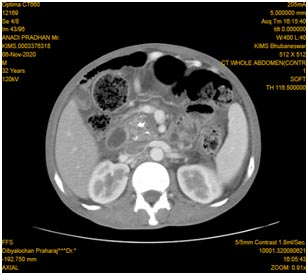
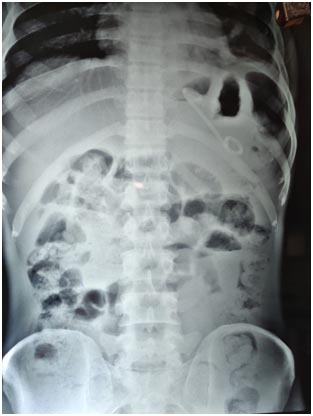
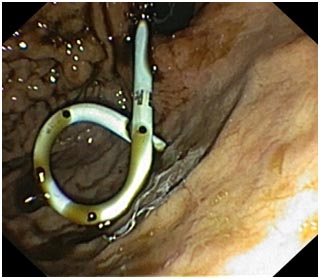
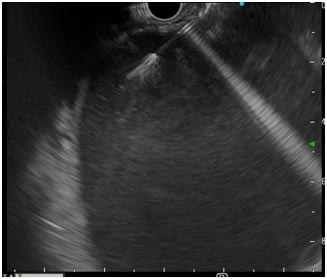
The splenic vein was thrombosed with multiple perigastric collaterals and there were three peripancreatic pseudocysts of size 11.3 × 6.0 cm (TR ×AP), 7.0 × 3.7 cm (TR × AP), 11.4 × 11.2cm (TR × AP) (fig 2). Chest X-ray showed left pleural effusion with high amylase and lipase levels suggesting pancreatic pleural effusion. Upper gastrointestinal endoscopy showed a bulge of pancreatic pseudocyst in fundus. Endoscopic ultrasound (EUS) guided cyst cavity was punctured with cystotome (fig 3) and the tract was dilated gradually with balloon upto 12 mm. One double pigtail plastic stent of 10 f x 5 cm(fig 4) was placed as the content of the cyst cavity was mostly liquid without any necrotic debris.
Post-procedure pain abdomen gradually subsided, appetite improved and follow up trans-abdominal ultrasound showed complete collapse of two pseudocyst along with reduction in size of third pseudocyst with resolution of pancreatic pleural effusion (fig 5). The patient was discharged in two days post-procedure with pancreatic enzyme replacement therapy.
Earlier patients with disconnected pancreatic duct syndrome were managed with surgery with a high risk of morbidity and mortality. With advancement of endoscopic techniques these patients can be safely managed with minimally invasive techniques like EUS guided cysto-gastrostomy. Using EUS also decreases the chance of bleeding as these procedures are performed under real time image, especially helpful in patients with perigastric collaterals due to splenic vein thrombosis like our patient. The stent has to be left for an indefinite period in presence of disconnected pancreatic duct syndrome which is safe.